
Partnership has always been essential to achieve healthcare's aims. And where there's a will — and a pandemic — there's a way. To find the way, hospitals and community-based organizations must partner in new ways to incorporate social determinants of health into patient care improvement efforts. Rich new SDOH data sets can supercharge the design, implementation and evaluation of SDOH initiatives as providers are expected to assume more responsibility for outcomes related to non-clinical factors.
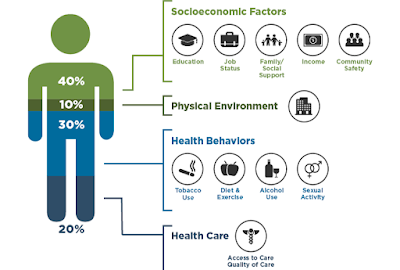
The impact of social determinants of health
People naturally understand it is harder for someone to manage their diabetes without access to affordable, healthy food. Through the federally-required Community Health Needs Assessment process, hospitals understand local need, but many do not yet know how to shift from a longstanding clinical focus to incorporating SDOH into program design and total cost of care. The coronavirus pandemic has forced a rapid pivot in this direction that would have otherwise taken years to achieve.
Managing total cost of care is essential for value-based care and to achieve healthcare's Triple Aim: better population health management, patient experience and cost control. But the Triple Aim has never explicitly included health equity. A January 2022 article from the Journal of the American Medical Association has called for this very thing, stating, “It is tempting to argue that health equity is already covered in 2 of the aims, better experience of care and better health for populations. But neither is guaranteed unless health equity is made an explicit goal.” The authors add that “quality improvement without equity is a hollow victory.”
With providers now called upon to be a proactive part of SDOH solutions, hospitals and health systems are in a unique yet challenging position to make a difference. Their charge is to support health equity through program sponsorships, collaboration, education and advocacy, all informed by new SDOH data and analytics resources.
The unique role (and challenges) of hospitals and health systems
It doesn't take an exponential funding increase to get started. Even before funding is identified, communication and partnership with community-based organizations are vital and must be guided by what DataGen defines as the Discover-Plan-Act cycle.
The “Discover” phase involves gaining insights using reliable sources of data and proven methods of analysis. A base of meaningful analysis can serve as a tool and prelude to working with CBOs. As the JAMA article puts it: “Quality improvement efforts should . . . [involve] persons from groups and communities that are affected in the planning, designing, and delivery of interventions so they are inclusive, culturally sensitive, and structurally appropriate.”
Please stay tuned. In our next blog, we will further explore how to take the next steps through high-quality alternative SDOH data sources.
Comments
Post a Comment